


006. Zuranolone from a Pharmacist & Severe PPD Survivor's Perspective
The medication I wish I had the option to consider, 4 years ago


Two weeks ago, on August 4, there was a huge buzz in the perinatal mental health world about the FDA approving the first pill indicated for treating postpartum depression (PPD)—Zurzuvae (zuranolone). I know there will be more weigh-in on this later on because this is still so new. But I know some followers wanted to hear more about it from my stance as a clinical pharmacist—and especially as someone who survived severe postpartum depression. Because this pill is specifically tested in and indicated for severe PPD.
Let’s back track a little and be clear that this is not the first medication ever to be indicated for postpartum depression. There was another medication that was approved in 2019, right before I gave birth to my daughter—Zulresso (brexanolone). It was so new back then that I didn’t even know about it when I was going through the depths of my severe PPD, just a few weeks fresh from becoming a new mom.
In fact, I didn’t even learn about brexanolone until over a year postpartum when a pharmacist friend I went to school with asked me if I had ever heard of or considered it. Truthfully, the drug wouldn’t have been even available to me in the deepest depths of when I needed treatment at the time. And I think my insurance wouldn’t have even covered it until after I had tried and failed at least 4 different antidepressants or something of that nature.
I think in order to discuss and understand the new buzz drug and why it’s such a breakthrough, we have to also compare it to brexanolone, which actually was the first medication indicated for PPD. So I’ll briefly go over what brexanalone is and then dive more into zuranolone.

What is brexanolone?
Zulresso (brexanolone) was made by the same company that developed the new pill Zurzuvae (zuranolone)—Sage Therapeutics. The FDA approved it mid-March 2019. It’s a one-time medication, but given via a 60-hour IV infusion, which basically means a 3-day inpatient stay at a hospital that will administer it. Can you see the dollar signs adding up? It costs around $34,000 for a treatment, per many news articles last week, and only 1000 patients have received it thus far, per Sage.
Brexanolone is a “synthetic version of allopregnanolone.” Allopregnanolone is what natural progesterone is metabolized to, and it has neuroprotective and anti-inflammatory effects. Low levels of allopregnanolone have also been associated with depressive symptoms in certain menopausal women too. (Hutner et al, 2020—see Resources at the end of this newsletter.)
Brexanolone is a “positive allosteric modulator of the GABAa receptors." The GABA system is a major inhibitory system in the central nervous system. Effects at GABAa lead to sleepiness, anti-anxiety, and anti-seizure effects. (Hutner et al, 2020) This mechanism likely explains its biggest side effect warning of excessive sedation and loss of consciousness, which is another reason why you can only get Zulresso through a restricted REMS program (Risk Evaluation and Mitigation Strategy).
Basically, this is a novel drug and first of its class in mechanism that some are calling “neurosteroids” and it does not work like a traditional antidepressant on the serotonin, norepinephrine, or dopamine systems.
In the two placebo-controlled studies for this drug, there was improvement in depression from baseline symptoms at the end of a 30-day follow up period.
Two Augusts ago (2021), I did an IG Live with a mama (some of you know her at Jenn of @momsmaternalhealth back then) who actually did do the brexanolone IV infusion herself. If you’re interested in hearing about the first-hand experience of getting this particular medication, you can find it on my IG Live archives—skip to minute 11 to start.
What is zuranolone?
Zuranolone is an oral pill cousin of brexanolone, which is very exciting because there are so many barriers to getting the 60-hour IV infusion version that is highly regulated by REMS. So zuranolone is the first oral medication indicated for postpartum depression, which makes it very exciting.
Zuranolone typical dosing will be 50mg orally once daily with a fatty meal for 14 days and then stopped.
The Sage Therapeutics business update slides from last week also mention it will come in 20mg, 25mg and 30mg tablets, with option to reduce to 40mg if there are CNS depressant side effects. (See resources below for link.)
How does zuranolone work?
Similar to brexanolone, zuranolone likely also works at GABAa receptors as a positive modulator and a synthetic version of allopregnanolone. As mentioned above with brexanolone, allopregnanolone is what natural progesterone is metabolized to.
After a baby is delivered, levels of estrogen and progesterone will drop off pretty drastically. This change in hormone levels can be one potential cause for postpartum depression, but even more especially because of a lower level of available allopregnanolone that can act on the GABAa receptors. Again—sleepiness, anti-anxiety, and anti-seizure effects.
What do the studies say about zuranolone?
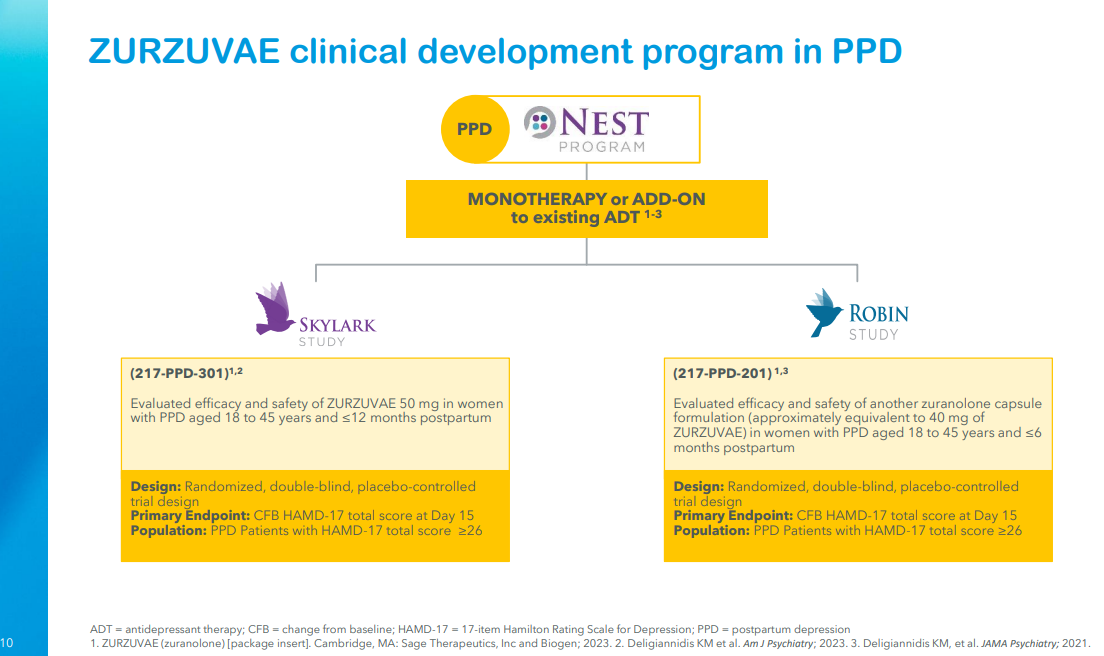
Two randomized, double-blind, placebo-controlled studies were done on zuranolone, named SKYLARK and ROBIN, which have been published in pretty large psychiatry journals.
You can see some of the details in the slides below, but basically they looked at postpartum women who scored as severe depression on the Hamilton Depression Rating Scale (HAMD-17) at baseline and looked at their change in scores throughout the treatment. The primary endpoint was at day 15 after the medication period was over, and they also looked at scores up to 45 days after initiation of treatment. The two studies differed slightly in the dosing (zuranolone 50mg vs zuranolone 40mg) and time periods of postpartum (<12 months or <6 months postpartum).
One thing I noted in the studies was that patients enrolled had to have onset of PPD in the third trimester of pregnancy up to 4 weeks postpartum at the latest. This narrows the window a bit of diagnosis since we know PPD can be a higher risk during the entire first year postpartum, and many incidences do not occur until after 4 weeks postpartum.
In both study populations, the majority was white (50-70%), followed by African American, and very little other minorities represented. Patients with a history of bipolar disorder, psychotic disorders, attempted suicide, or risk of suicide in the current episode of PPD were also excluded.
To give some more clinical context, on the HAMD-17 screening tool used in the study, this is how you would classify scores:
0–7: normal
8–16: mild depression
17–23: moderate depression
>24: severe depression
So enrolling people with scores over 26 would have been patients who were classified as severe PPD. The screening has a maximum score of 52.

The results show that there was statistical improvement in scores even on day 3 and especially at day 15, the primary endpoint. They also saw continued sustained decreasing scores even at day 45 of follow up that were statistically significant.
As far as clinical significance, I admit I don’t know the HAMD-17 screening enough to comment, but even in the sub-analyses I dug into, I noticed EPDS scores improved better than placebo group too.
It’s pretty exciting that even after a few days there is improvement, though, because traditional antidepressants would not work that fast!
Why is there such a buzz around zuranolone?
Besides for being the first oral treatment of its kind, the fact that there are indications for “postpartum depression” is huge. Wendy Davis, executive director of Postpartum Support International said in a NY Times article that the indication itself raises awareness that there can be biological causes for PPD and helps to destigmatize it for women all over.
I personally think that the dosing and route are convenient, which will make this a more practical medication for postpartum women to take. The fact that there are quick results and improvement is also something desirable. It’s a major factor that zuranolone is only taken for 14 days and then stopped because traditional antidepressants like SSRIs and SNRIs work on serotonergic pathways that can take 4-6 weeks to work—and that’s if it’s the right dose!
Not only does it take a long time to titrate to the right dose, but traditional antidepressants also take a lot longer to wean off and should not be stopped cold turkey. So zuranolone offers a great option for mothers with severe PPD who might need relief faster and feel like a two-week period could be worth trialing.
The mechanism of action is also fairly new (taking after its cousin brexanolone), and it further highlights that some (not all) roots of PPD are biological and hormonal. The fact that zuranolone was NOT approved for major depressive disorder also further shows how postpartum depression is a slightly different disease of its own.

What else is there to consider, and what’s next?
Zuranolone has not been tested on pregnant women. Since it works on a hormonal pathway that may be affected during postpartum, I’m not sure if it will work well on pregnant women anyway. Additionally, animal studies showed risks of fetal harm, and I’m not sure this medication will be tested on pregnant women.
It is also not advised for breastfeeding women to use it, so women who take this may have to stop nursing for the 14 days they are on it before resuming afterwards. However, the 14 days is better than waiting 4-6 weeks on traditional antidepressants. A small lactation study done with 14 healthy lactating women showed relative infant dose (RID) of 0.375%, per package insert. Typically, RID <10% is considered relatively safe.
I’d also love to see more studies of longer follow up. Follow up at 45 days after taking the medication is longer than the 30-day follow up on brexanolone, but it’s still not enough. I’m curious how long the effects of zuranolone will carry on for and if women can stay in remission for that whole year postpartum. And I would love to see more detailed data on how zuranolone is used as monotherapy (single medication only) or adjunctive therapy (add on) to traditional SSRIs. It’s indicated for both right now.
As a more personal hope, I would also love to see larger studies that include more women of color, including AAPI women. I know this can be hard to conduct, but women of color have poorer outcomes when it comes to maternal mental health, so anything done to study it would be immensely valuable research.
Currently, the FDA has a 90-day review period before zuranolone can be available. It also is pending a controlled substance scheduling.
Would I have considered taking zuranolone?
Short answer: yes.
I know when I was asked to take an SSRI (Zoloft) by my OB/GYN at my 6-week postpartum check, I was resistant to the idea. As a pharmacist, I already knew how long it would take to have effect. To me, I didn’t have the time to wait 4-6 weeks for a medication to work—and I knew the dose would have to be titrated too, so we were looking at a few months before seeing results.
I was desperate and panicking due to insomnia and exhaustion. I needed relief yesterday. In other words, I had already labeled myself as hopeless, which didn’t help but feed into the vicious depression feelings of worthlessness.
So a 2-week medication? I definitely think my doctors would have had more of a chance in convincing me to try something for 2 weeks than waiting to titrate the Zoloft up. Not to mention, because I had a lot of insomnia and sleep issues that contributed to my severe PPD, zuranolone’s side effect profile actually would have been a good option for me. (The biggest side effects of zuranolone include sleepiness, dizziness, and confusion.)
Additionally, something labeled specifically for PPD might have also helped me to really put a name to the disease, even if I knew deep down that I had depression. To have others validate and vet postpartum depression as a diagnosis worth treating would have been de-shaming in a way. Like my psychiatrist always says, if you were given a diagnosis of cancer, wouldn’t treat it aggressively? Why not treat your mind then?
In the Perinatal Mood Disorders training I did last week from Postpartum Support International (PSI), one of the quotes that stood out to me was, “Is your head not attached to your body?” In other words, we worry so much about taking care of our physical body, why wouldn’t we also give our mental health the same attention and care it deserves?
I will be frank: medications can be scary. I don’t think it’s for everyone. And I’m not here to push it. Actually, pharmacists are probably the least likely to want to take medications. I talk about it though, because I want to destimatize it and show that it can play a significant role in healing. Therapy is still needed and should definitely be woven in.
But when I read Karen Kleiman’s This Isn’t What I Expected, she mentioned that severe cases of postpartum depression tend to respond better to medications. And knowing what I know now in the aftermath, as new as this medication is, I would have loved to try it and see if it made a difference in my recovery.
Time is precious, and I think that’s the biggest loss during PPD. So if zuranolone can save some time and help mothers get better quicker, I’m all for it. But I always emphasize that medications won’t cure you. You still need to put in the work; they just clear the path for you to do the work.
Again, this is just my own personal stance. I know we’re all individuals that have to be taken into account, so please don’t see this as me pushing it on anyone.

Closing Words and Other Resources
There’s still a lot of work to be done to support moms in the postpartum period. Zuranolone is only one option and might open a door for some women. It’s not perfect; neither are moms. Medications are not the only way to treat postpartum depression. But they’re not the bad guy here either.
I’ll include a few of the sources I used and/or found helpful for compiling this newsletter below if you want to look at more:
- newsletter
- newsletter
Textbook of Reproductive Mental Health, by Lucy Hutner, MD et al.
Sage Therapeutics Business Update Slides, August 7, 2023
Thanks for reading along if you did! I know it was really dense. But if you’re like me, I would want all the details I could glean. And if you like my writing, please consider sharing my newsletter with a friend or subscribing if you haven’t already! <3
Be well,
Jasmine
Thank you for this and for including Two Truths as a reference! 🤍